











































30 Years of Polio Campaigns in Ethiopia, India and Nigeria: The Impacts of Campaign Design on Vaccine Hesitancy and Health Worker Motivation
Johns Hopkins University Bloomberg School of Public Health (Neel, Closser, Villanueva, Kalbarczyk, Alonge); Indian Institute of Health Management Research (Majumdar, Gupta); Middlebury College (Krugman); University of Ibadan College of Medicine (Akinyemi); Addis Ababa University (Deressa)
"A focus on a single disease in a population underserved by the health system can lead to slow-burn opposition to a vaccine that takes time to arise."
Donor-driven, disease-specific ("vertical") programmes, including mass vaccination campaigns, have a range of impacts, both positive and negative, on health systems. That is, the health systems impact of a campaign is often distinct from the success (or failure) of the campaign itself. Health systems are complex and dynamic, with elements of the system affecting outputs and outcomes over time. This article uses a complex adaptative systems (CAS) lens to explore the relationships between polio campaigns (that is, oral polio vaccine (OPV) vaccinations delivered separately from routine immunisation, or RI) and health systems in Ethiopia, India, and Nigeria. Specifically, the analysis focuses on how interactions between the polio programme and the health system influence two key outcomes: frontline health worker (FLHW) motivation and vaccine hesitancy. These two factors, in turn, affect OPV campaign coverage itself.
This paper describes an analysis of qualitative data sourced from two studies. The Polio Eradication Impacts Study, conducted 2011-2012, explored the relationship between the Global Polio Eradication Initiative (GPEI), RI, and primary health care through 175 interviews conducted with policymakers, officials, and frontline staff in seven study sites. The Synthesis and Translation of Research and Innovations from Polio Eradication (STRIPE) study, conducted in 2019, used 101 interviews to map explicit and tacit knowledge from polio eradication at the global level and in seven countries. The researchers constructed a causal loop diagram (CLD) from analysis of semistructured interviews drawn from both studies in three countries: Ethiopia, India, and Nigeria.
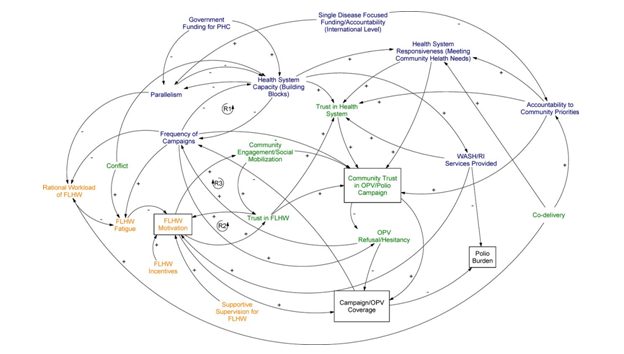
The CLD (see above) shows how campaigns interact with health systems over time to affect system outcomes (e.g., FLHW motivation), and the effects of those system-level outcomes on polio programme outcomes (e.g., OPV campaign coverage). A positive arrow (+) means that an increase in variable A will lead to an increase in variable B. A negative arrow (-) indicates that an increase in variable A will lead to a decrease in variable B. An increase in the frequency of polio campaigns, for example, increases (+) health worker fatigue, whereas a reasonable workload for FLHWs reduces (-) fatigue. The CLD shows simultaneous causation, where variable A can cause variable B, and variable B can also cause variable A at the same or different times. This is depicted as a feedback loop. In a reinforcing loop (e.g., the link between health worker motivation and trust), the links between the variables move in the same direction, creating an amplifying effect (when health workers are trusted, they are more motivated, leading them to act in ways that further reinforce trust). Multiple pathways may exist between one variable and another: For example, the relationship between FLHW motivation and OPV coverage can operate through community engagement, trust in the FLHW, or directly.
The analysis divides the CLD into three sections, providing examples from Ethiopia, India, and Nigeria:
- Policy level - The GPEI's single-disease focus impacted outcomes through two main pathways: (i) through the construction of parallel systems to deliver polio vaccination through single-disease campaigns, rather than by improving RI and water, sanitation, and hygiene (WASH) infrastructure over the long term; and (ii) through pushing health systems to focus on global agendas, reducing accountability to community priorities and responsiveness to community needs.
- FLHW or service delivery level - Strategies like frequent campaigns were often quite effective in the short term, but over years, especially when combined with poor incentives and lack of supportive supervision, drove worker fatigue in powerful and at times corrosive ways. In contrast, highly motivated workers contributed to more effective and sustained community engagement. Across place and time, effective community engagement, carried out by motivated workers, led to greater levels of community trust in the workers themselves and, by extension, the vaccination campaign.
- Community level - The CLD represents how vaccine hesitancy is integrally tied to health systems dynamics. Trust in polio campaigns was powerfully shaped by communities' trust in the health system more broadly. When health systems were generally not accountable to community priorities, people questioned why polio vaccine was delivered to their doorstep. In some cases, lack of accountability to community priorities led to OPV refusals that were strategic: that is, people trusted the polio vaccine, but they refused it in an attempt to get the government to provide them with services they needed. Nigeria is an example of this, as are Pakistan and Afghanistan, which in recent years have experienced an increase in "demand refusals" and risks for FLHWs.
Thus, pursuing high coverage in polio campaigns without considering the dynamic impacts of campaigns on health systems, cost campaign coverage gains over time in weaker health systems. Over time, the systems effects of frequent campaigns, delivered through parallel structures, led to a loss of FLHW motivation and an increase in vaccine hesitancy. (In stronger health systems with fewer campaigns, these issues did not arise.)
The researchers reflect: "A key dynamic here is power: who has the ability to set agendas for communities? Where power is applied to push through a specific vaccination agenda when frontline workers and communities have different agendas, resistance will arise....[In] fact, demand refusals are not really hesitancy: they are organised resistance to the application of power."
In all the study countries, community resistance of this nature was mitigated through co-delivery of health interventions, which encompassed a suite of ways to increase responsiveness to community needs even while operating within the confines of a parallel vertical programme. In Ethiopia and Nigeria, OPV was increasingly delivered alongside vitamin A, insecticide-treated nets, and deworming tablets, and CORE Group Polio Project volunteers engaged Indians in child health education.
In light of this analysis, the researchers suggest that mass vaccination campaigns, including COVID-19 vaccine campaigns, should plan for both worker fatigue and vaccine hesitancy over the long haul if multiple and frequent mass campaigns are not integrated with broader health system activities. Co-delivering other interventions in mass vaccination campaigns is a key way to minimise negative dynamics when relying on parallel structures is unavoidable. At a minimum, an intervention that is not addressing a community priority should be paired with one that is.
In conclusion: "Ultimately, for health campaign designs to be effective, they must make sense for those delivering and receiving campaign interventions, and must take into account the complex, adaptive nature of the health systems in which they operate."
BMJ Global Health 2021;6:e006002. doi:10.1136/bmjgh-2021-006002. Image credit: © Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
- Log in to post comments