











































Vaccine Hesitancy: Clarifying a Theoretical Framework for an Ambiguous Notion
INSERM, UMR912 (SESSTIM) - Peretti-Watel, Ward, Verger; Aix Marseille University UMR_S912, IRD, (Peretti-Watel, Ward); London School of Hygiene and Tropical Medicine (Larson, Schulz); ORS PACA, Southeastern Health Regional Observatory (Peretti-Watel, Verger); Université Paris Diderot (Ward); Inserm, F-Crin, Innovative Clinical Research Network on Vaccination (Verger)
"VH is an ambiguous notion and its theoretical background appears uncertain. It may have originated as a catchy expression coined by experts to capture policy-makers’ attention, as current vaccine coverage rates do not yet reflect the growing reluctance toward vaccination witnessed by empirical researchers. But hasty use of this notion may lead to misunderstandings and ineffective policies..."
This paper explores the meaning of "vaccine hesitancy" (VH), a term increasingly being used in the public health literature to describe the spread of vaccine reluctance. According to the Working Group on Vaccine Hesitancy appointed by the World Health Organisation (WHO)'s Strategic Advisory Group of Experts (SAGE) on Immunisation, VH refers to "delay in acceptance or refusal of vaccines despite availability of vaccination services", which is a phenomenon that is "is complex and context specific varying across time, place and vaccines". VH has been defined as a set of beliefs, attitudes, or behaviours, or some combination of them, shared by a large and heterogeneous portion of the population and including people who exhibit reluctant conformism (they may decline a vaccine, delay it, or accept it despite their doubts) and vaccine-specific behaviours.
The authors begin by reviewing current definitions of VH like this one and examine its most prominent characteristics. They then underline some of the ambiguities of this notion and argue that it is more a catchall category: "VH is not really an empirical concept, as the term 'concept' traditionally refers to a general mental representation derived from the variety of perceived objects and defines what is common to them - the features necessary and sufficient for membership in the class/concept - through comparison, reflection and abstraction. The current definitions of VH, rather than delineating a set of core elements, cover a wide range of heterogeneous, and even sometimes contradictory, elements." For example, those who consider VH an old phenomenon that encompasses anti-vaccination attitudes often attribute it to ignorance, misinformation, or irrationality, while those who describe it as a new attitude, distinct from strong opposition to vaccination, argue that it is positively correlated with vaccine-related knowledge.
The authors next explore VH's qualification as a belief, attitude, or behaviour. They suggest that we consider VH as a decision-making process (how/why do people come to accept/refuse/delay vaccination) that is influenced by various contextual factors (e.g., "local vaccination cultures"), which leads to a variety of behavioural outcomes. They call into question the usefulness of understanding VH as an intermediate position along a continuum ranging from anti-vaccine to pro-vaccine attitudes, saying: "although VH can be considered to be an intermediate position between the pro- and anti-vaccine positions in terms of vaccine assessment (positive/negative), it is not in terms of the decision-making process. Moreover, a still different group, those with no definite opinion, little knowledge and little interest about vaccination issues and who randomly forget or delay some vaccines, share the same intermediate position on the anti/pro continuum, but they show the same behavioural pattern as people who are uncertain but very interested and committed in vaccination issues, prone to information seeking and long and balanced decision-making. In other words, the behavioural outcomes generally associated with VH may reflect the genuine inconsistency of uncommitted people, as described above, but may also reflect a decision-making process that is not guided by a general attitude toward vaccination, but that instead takes the specificities of each vaccine/context into account, among people strongly committed to vaccination issues."
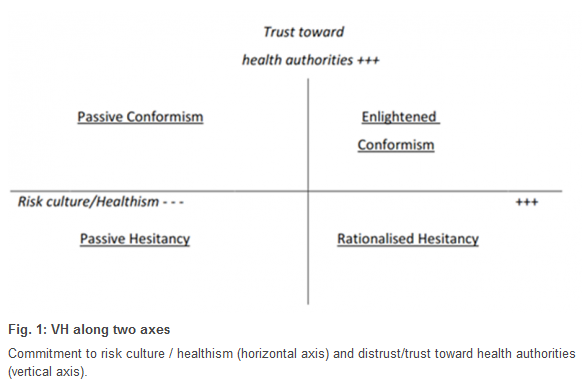
Finally, they propose a theoretical framework that considers VH as a process that depends on people's level of commitment to "healthism/risk culture" and on their level of confidence in the health authorities and mainstream medicine. It distinguishes two very different kinds of VH: first, that of people with poor knowledge of and indifference to vaccination issues and erratic vaccination behaviours, and, on the second hand, that of people who are very interested and committed to vaccination issues and prone to information seeking and long and balanced decision-making. "From a psychological point of view, this axis echoes the notion of locus of control: some people believe that they can control events related to their life (internal locus of control), while others endorse a more fatalistic attitude, tending to believe that their life is driven by forces outside themselves (others, fate or luck: external locus of control)." The authors discuss "the trust issue", which is generally considered a crucial component of people's attitudes toward vaccination, including VH. For example, people who endorse risk culture and decide to take their health in hand are confronted with discordant sources of knowledge, so they may distrust "official" sciences and experts, instead putting their faith in "alternative" sources of information or medical practice (such as homeopathy or acupuncture).
Figure 1 illustrates VH in a 2-dimension map, whose 2 axes can be used to represent different types of VH. This framework abandons the anti/pro vaccination continuum. It also underlines that, "although health promotion policies aiming at encouraging people to take their health in their own hands may move people further along the horizontal axis, health promotion may nonetheless fuel VH, at least among some populations, unless they are positioned high on the trust axis."
The authors conclude with several suggestions for future research; for instance, studying the interactions between the various participants involved in immunisation policies, from public health experts to lay people, asking questions such as: Is there a "hesitancy cascade", with waves of influences from political hesitancy to provider hesitancy to public hesitancy, and is there a feedback effect in some cases (patients' VH reinforcing physicians' VH, which in turn fuels VH among other patients)?
PLOS Currents: Outbreaks collection, accessed November 24 2015.
- Log in to post comments