











































Leading from the Frontlines: Community-oriented Approaches for Strengthening Vaccine Delivery and Acceptance
"Policymakers, researchers, and local organizations should adopt local approaches to provide communities both a voice and resources to turn their needs and ideas into action. This comprehensive approach can amplify local voices, identify local concerns and advocates, and leverage 'bottom-up strategies' to co-design successful interventions to facilitate long-term change."
Vaccine hesitancy, defined as a delay in acceptance or refusal of vaccines despite the availability of vaccination services, along with structural and systematic pandemic-related disruptions, have taken a toll on vaccine coverage globally. Community ownership is an approach to these issues that strives to empower all members of a community, including community health workers (CHWs), community leaders, parent and child caregivers, and others, to take a leading role in developing strategies and coordinating interventions. From VARN2022: Shaping Global Vaccine Acceptance with Localized Knowledge, this paper outlines the Community Health Worker-Led Intervention for Vaccine Information and Confidence (CIVIC) Project, which aimed to leverage CHWs' local expertise and strengthen their role in vaccine uptake in Mewat District in Haryana, an area in India with extremely low vaccination coverage.
The research team of Johns Hopkins Bloomberg School of Public Health (JHSPH) and Bal Umang Drishya Sanstha (BUDS) used a 5-state process, leveraging community-based participatory research to closely involve the community from conception to implementation of the community-level intervention.
- Development of community accountability board (CAB): Ten influential community members, including senior CHWs, religious leaders, teachers, sarpanches (council leaders), and village elders, were identified and recruited to assist with providing perspectives on community acceptance of vaccines, be involved in the design of the intervention, and meet on a monthly basis to discuss the progress of the project.
- Pre-intervention data collection and analysis to design prototype intervention (January and February 2021): The JHSPH-BUDS team conducted qualitative in-depth interviews with CHWs and CAB members and completed 30 baseline surveys with mothers, fathers, and grandmothers. The data that emerged highlighted communication barriers associated with vaccination activities, ranging from senior CHWs not providing frontline CHWs with sufficient knowledge to communicate with parent and child caregivers, to parent and child caregivers feeling that their concerns were being neglected in the push to rapidly meet vaccination targets set by district and state-level health officials.
- Refinement of the intervention prototype through two human-centred design workshops (March 2021): The CHWs and CAB members who were interviewed in Phase II led the design of materials they felt was missing from the preliminary prototype of a multi-pronged intervention that was designed to motivate and sustain long-term vaccine uptake by addressing the most prominent rumours, misconceptions, and barriers that were identified in the preliminary data collection.
- Implementation of the intervention (April 2021), with ongoing monitoring: After the HCD workshops and feedback from CHWs and CAB members, the team refined and created an updated intervention that focused on:
- Involving religious leaders in vaccination efforts - The team worked closely with religious leaders to address their vaccination concerns, encourage their involvement in CAB meetings, and motivate them to participate in vaccine advocacy. They then agreed to participate in the remainder of the intervention and serve as vaccine champions.
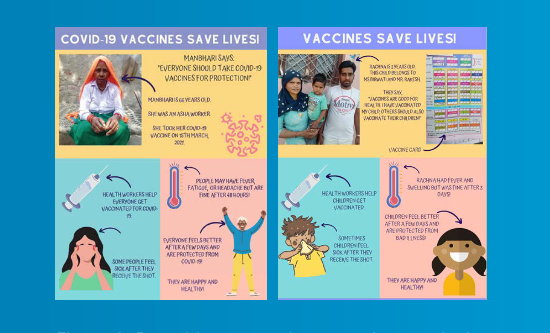
- Designing pamphlets and videos that could be used by CHWs to initiate and facilitate discussions with parents and caregivers - Pamphlets addressed the most prominent issues perceived in the community, and they used language that was most appropriate for the parent and child caregivers in this setting. Largely pictorial, these pamphlets displayed well-known and influential members of the community who had received vaccines themselves, or who had vaccinated their children. In addition, the three videos of respected community members who were willing to advocate for vaccines included both religious leaders and members of the CAB. Videos were designed to be short, easy-to-use in conversations with parent and child caregivers, and easy to disseminate on WhatsApp among parent and child caregivers. The videos also filled the literacy gap highlighted in the HCD workshops.
- Addressing the CHWs' communication and knowledge gaps that were identified in earlier phases of the project - The trainings were designed to distill complex topics, which CHWs had not previously had exposure to, into easy-to-digest material. The team further ensured that walkthrough exercises provided CHWs with opportunities to practice these new skills.
- Working with senior CHWs to address parent and child caregiver and CHW concerns that there was not sufficient time to ask or answer questions about vaccines on vaccination days - For example, senior CHWs provided advance notice to CHWs for vaccination days so CHWs could, in turn, speak with parent and child caregivers early.
- Post-intervention data collection and analysis: During the monthly CAB meetings, the team made the following additions to strengthen the intervention: (i) They included maulanas (Muslim scholars) in the CAB as opposed to requesting them to serve as advocates; (ii) they created an additional video of a maulana advocating for vaccines; (3) CAB members began to assist CHWs with reaching out to hesitant parent and child caregivers during CHWs' door-to-door visits; and (iv) CAB members began to attend vaccination clinics to instill vaccine confidence in parent and child caregivers.
After completing the intervention, the team found that parent and child caregivers had improvements in their knowledge of the purpose of vaccination and on side effects of vaccines. Parents and caregivers also noted that the involvement of community and religious leaders in vaccination efforts was welcome. Furthermore, parents and caregivers expressed that they were more willing to travel to vaccinate their children, and they had fewer non-logistical reasons to refuse vaccination services. Interviews with CHWs and CAB members stated that they felt greater ownership over vaccination in their community, and CHWs felt more prepared to address community concerns with routine and COVID-19 vaccine misinformation. However, CHWs and CAB members noted that additional gaps remained.
In conclusion, by building on community-based participatory research strategies, the team was able to "create networks to support more discussions about vaccination as well as facilitate parent and child caregiver self-efficacy to access and accept vaccines....To create long-lasting solutions to vaccine barriers, researchers should begin by engaging deeply with the community to identify barriers and facilitators to vaccination. Researchers should then partner with the community leaders, as they are the local experts, to prototype and refine an intervention tailored to the vaccination needs of the community....Lastly, it is essential to support community leadership, such as a CAB, to develop and sustain a successful health intervention beyond the period of the project."
- Log in to post comments