












































How Should Home-Based Maternal and Child Health Records Be Implemented? A Global Framework Analysis
University College London Medical School, and Royal Free London NHS Foundation Trust (Mahadevan); University of Colorado Anschutz Medical Campus (Broaddus-Shea)
"Optimizing implementation of HBRs can potentially increase ownership and equity of coverage and improve engagement with the HBR content."
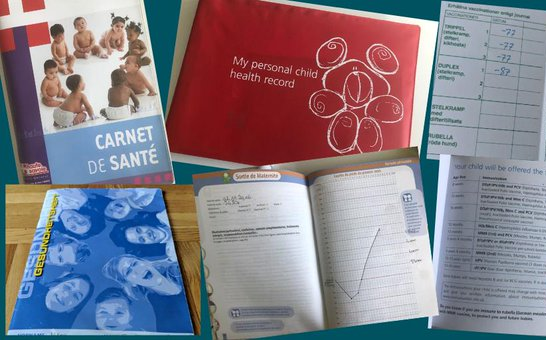
Initially introduced in immunisation programmes, home-based records (HBRs) can take many forms in the 163 countries in which they are used, including antenatal care records, vaccination-only cards, vaccination-plus cards or booklets, child health books, and combined maternal and child health (MCH) books. There is evidence that HBRs can improve patient-provider communication, support continuity of care, and empower women and children by encouraging them and their caregivers to be health literate and actively participate in their own care. Using a framework analysis approach, this study sought to delineate the facilitators and barriers to the effective implementation and use of HBRs, especially in low- and middle-income countries (LMICs). This study was part of the evidence synthesis for the World Health Organization (WHO) recommendations on HBRs for maternal, neonatal, and child health (MNCH).
The researchers drew on 18 gray literature documents and 12 semi-structured interviews with key informants (with a breadth of experience, predominantly in LMICs), abstracting the relevant data into an analytic matrix. They identified 8 main components of the implementation process, all of which are envisioned as spokes of the wheel of a successful HBR programme:
- Establishing high-level support: Many of those interviewed highlighted that strong advocacy is required to educate government stakeholders, particularly health ministry officials, and donor and coordinating agencies about the benefits of an HBR programme and what is required to implement it. Respondents identified robust evidence about HBRs to be a prerequisite for such advocacy.
- Coordinating partners: Multiple sources noted that all partners involved in implementing the HBR programme needed to frankly discuss their individual priorities at the start of the process to ensure they were on the same page and committed to creating harmonious HBR content rather than competing with each other.
- Selecting HBR contents: International and ministry-level respondents with policy experience in multiple countries indicated that the HBRs had the dual purposes of recording health parameters and communicating health education messages. However, many respondents viewed them only as recordkeeping tools; they suggested training healthcare workers to use the HBR as a starting point for health education conversations as well.
- Designing HBRs: Interviewees unanimously agreed that the design process should involve community and end user input, so as to ensure that the HBR is mindful of local cultural sensibilities and aligned with workflows, making it more likely to be used. Respondents explained that it was important for regional languages to be represented on HBRs, not just the official or national language/s. Many sources noted the importance of adapting HBRs for low-literacy populations by using pictorials and rigorously testing these to ensure they conveyed the desired message.
- Covering costs: Many sources preferred early planning for a gradual transition from donor to government funding, and they noted that this planning was made easier when the government/Ministry of Health was empowered from the start to lead the process.
- Printing and distributing HBRs: Multiple sources found printing and distribution to be where the most roadblocks occurred. One respondent noted that rural and remote regions and those with large transient populations (e.g., refugees) posed particular challenges - both in terms of estimating numbers and in terms of HBRs and other services practically reaching them.
- Promoting HBR use among healthcare providers: Sources explained that initial training on using the HBR must be given at the local level to all healthcare workers in both the public and private sectors who deal with HBRs. Refresher training was deemed especially useful for community health workers, who tend to have less formal education but who are vital in engaging rural or disenfranchised women/caregivers with the HBR. One suggestion was to reward healthcare workers who complete the most HBRs in practice.
- Promoting HBR use among pregnant women/caregivers: Many documents and nearly all respondents spoke about the importance of patients/caregivers being introduced carefully to the HBR when they received it for the first time, with an explanation of its value and the necessity of bringing it to every health visit. Involving health professionals, such as community health workers and midwives, and nonhealth-sector stakeholders, such as religious and community leaders, in HBR pretesting and promotion was also viewed as important for gaining the acceptance of end users and making HBRs more relevant to them.
There are multiple interlinkages between these 8 implementation components. For example, the content areas chosen and the design of the HBR affect how it is valued and used by healthcare providers and pregnant women/caregivers. On that note, the researchers indicate that a number of existing studies have affirmed the importance of the design of the HBR. Sources advocate for plastic covers for physical durability, simple uncluttered layout, large print size, nontechnical language, attractive colours and shading, and clear photos or illustrations. Incorporating these changes when redesigning immunisation cards contributed to improving childhood immunisation adherence in studies in both urban and rural Pakistan.
The researchers call for further research on the perspectives and motivations of healthcare workers who deal with HBRs and on how HBRs can be effectively integrated with existing facility-based health information systems. Research is also needed, they suggest, on the differences between implementing single-focus and multiple-focus HBRs, including whether their unique characteristics make them suited to different contexts or populations.
In conclusion: "The hope for the related WHO guidelines...is that policy makers, donors, and the end users of HBRs (frontline health care providers, pregnant women, and the families of children) will all be able to better harness the benefits of HBRs for improved MNCH outcomes, increased participation and shared decision making, and better coordination and continuity of care."
Global Health: Science and Practice March 2020, 8(1):100-113; https://doi.org/10.9745/GHSP-D-19-00340. Image credit: WHO
- Log in to post comments