











































Determinants of Policy and Uptake of National Vaccine Programs for Pregnant Women: Results of Mixed Method Study from Spain, Italy, and India
International Vaccine Access Center, Johns Hopkins Bloomberg School of Public Health
"An organized voice and global and local champions can help raise political priority and action across all countries."
There are a number of reported reasons for the low coverage rates for maternal vaccination, decisions about which are influenced by a series of risk-benefit determinations. With the goal of sharing best practices across countries, this research focused on 3 countries - Spain, Italy, and India - to provide a diversity of situation, approach, and performance. Spain and Italy have similar recommendations for vaccinating pregnant women but different drivers of decisions and differing levels of uptake; India was selected to determine how a country's more limited national recommendations for maternal vaccination approaches decision-making and implementation differently.
The project used a mixed-methods approach, including a narrative literature review, desk research, and qualitative interviews to develop case studies to examine key factors influencing decision-making and uptake of maternal immunisation. The researchers reviewed 237 articles and conducted 59 key informant interviews between November 2018 and January 2019.
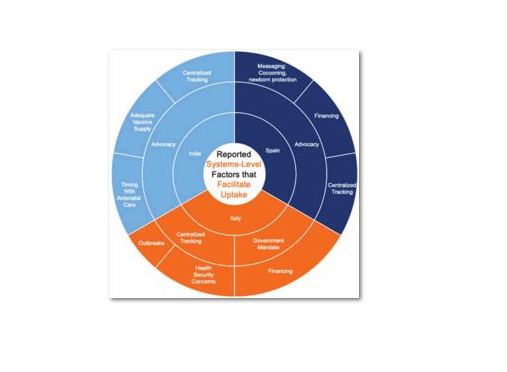
Both Spain and Italy recommend influenza vaccines and tetanus, diphtheria, acellular pertusis (Tdap) in pregnancy; India only recommends tetanus toxoid (TT) and had recently updated their recommendation to include tetanus-diphtheria (Td) as part of the national programme. India does not nationally recommend influenza vaccine for pregnant women, even for pandemic preparedness. Policies in Spain and Italy both reflect a life-course approach to vaccination, but recommendations and how they ensure uptake differs: Italy focuses on tracking of progress and mandates to ensure compliance in all regions, while Spain relies more on advocacy and efforts to build provider acceptance.
Looking more closely at the main drivers of decision-making, findings both from the literature review and interviews reveal that variance by country. For example, in Italy, elections and the influence of a female physician as health minister were mentioned as a driver of decisions. In fact, advocacy was described as a prime facilitator of uptake in Spain and India. However, the lack of physician buy-in amongst some was noted as a significant challenge in Spain. In India, maternal health advocates and those representing marginalised populations were deemed important, but many interviewees commented that providers, in general, were not making the recommendation, perhaps because they are not convinced due to a lack of local studies of vaccines in pregnant women. Some respondents questioned whether maternal health was a priority in India.
Hesitancy was noted by some respondents as a barrier to uptake for both women and providers in India and Italy.The issues with hesitancy described in Italy may stem from institutional distrust and political parties that tend to stoke these sentiments. However, respondents claimed that distrust and hesitancy around immunisation died down during outbreaks. Regional variation in hesitancy was also reported and, in every country, respondents noted the important role of providers, particularly obstetricians-gynaecologists (OB-GYNs), in convincing women to be vaccinated, although most felt they needed to be more proactive and that their influence could be strengthened.
Most respondents in all countries did not feel there was a champion for maternal immunisation to move the agenda forward. In general, respondents perceived the level of specific expertise in decision-making for pregnant women to be limited, and, in India, lack of data in pregnant women was a frequently cited barrier to decision-making.
Needs for improving rates of maternal vaccination include education of healthcare providers and pregnant women, use of central registries to track progress, stronger global guidance for use of vaccines, and engagement of champions, particularly OB-GYNs. As an example of the latter: The voices of OB-GYNs and midwives at the national level for maternal immunisation could be leveraged through a deliberate effort to engage OB-GYN and midwifery leadership in National Technical Advisory Group on Immunization (NTAGI) discussions and empower them to speak up through planned interactions with government officials and scientists to advocate for needed local data and evidence-informed decisions. In addition, health security concerns can be leveraged to build political priority.
A concluding suggestion: "Global monitoring of progress and stronger global guidance to strengthen platforms for maternal vaccination according to the needs of the country may help raise political priority."
Human Vaccines & Immunotherapeutics 2020. https://doi.org/10.1080/21645515.2020.1831858.
- Log in to post comments