











































Using the Journey to Health and Immunization (JTHI) Framework to Engage Stakeholders in Identifying Behavioral and Social Drivers of Routine Immunization in Nepal
JSI Research & Training Institute, Inc. (Castle, Oot, Elkes); Dhulikhel Hospital-Kathmandu University School of Medical Sciences (Kunwar, Joshi, Rai, Karmacharya); independent researcher (Khanal); UNICEF Nepal (Shrestha, Bhattarai)
"...demonstrates that there is strong demand for approaches and tools from behavioral science to use in relation to immunization and that this type of engagement model is effective for generating demand for and strengthening capacity to use behavioral science approaches."
Many studies have examined the socioeconomic determinants of vaccination and the demand- and supply-side barriers and enablers to vaccination in Nepal. However, none of the studies used a specific behaviour change model. Recognising that behavioural science offers promise in understanding the drivers of vaccination and in developing more effective, people-centred health programmes, the non-governmental organisation (JSI), the United Nations Children's Fund (UNICEF) Nepal, and the Dhulikhel Hospital-Kathmandu University School of Medical Sciences (DH-KUSMS) established a Behavioral Science Center (BSC) to engage a diverse group of stakeholders in increasing the capacity of practitioners to use behavioural science in immunisation programming. This paper describes the BSC's Behavioral Science Immunization Network, arguing that this type of engagement model is effective for generating demand for and strengthening capacity to use behavioural science approaches.
BSC members included representatives from government agencies, NGOs, academic institutions, and a professional society (Nepal Public Health Association). In consultation with the Ministry of Health and Population (MOHP), the BSC began its work by conducting formative research on the social and behavioural drivers of childhood vaccination in select wards in Kathmandu Metropolitan City and Sudurpaschim and Madesh provinces. The formative research process facilitated capacity strengthening of the DH-KUSMS core team and other BSC members, enabled the team to document the use of behavioural science tools and approaches in relation to immunisation, and supported stakeholder engagement and advocacy.
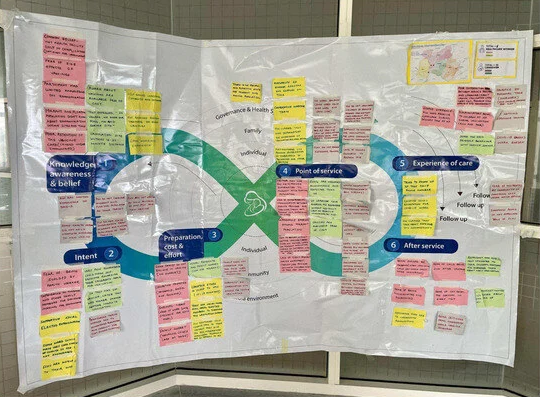
The team decided to use the Journey to Health and Immunization (JTHI) framework, a model and journey mapping tool developed by UNICEF and its partners in 2017 to enable practitioners to understand both caregiver and health worker journeys, providing insights into their experiences and challenges across six domains (see Figure 1 in the paper) that affect caregivers and health workers before, during, and after vaccination services are delivered. The JTHI is practice oriented, uses human-centred design (HCD) principles, supports problem prioritisation, and can be used to design tailored solutions to improve outcomes for individuals and communities, including those in low- and middle-income countries (LMICs) like Nepal.
Formative research was conducted using rapid inquiry in selected wards of Bagmati, Madesh, and Sudurpaschim provinces to understand the social and behavioural drivers influencing routine vaccine uptake. The BSC team conducted in-depth and key informant interviews with 52 caregivers (i.e., mothers, fathers, and/or grandparents of children between 6 months and 24 months of age) and 12 health workers and female community health volunteers (FCHVs). The BSC team adapted the Behavioral and Social Drivers of Vaccination (BeSD) guide using HCD tools and the JTHI to develop the interview guides.
Both the core DH-KUSMS team and BSC members participated in capacity strengthening throughout the formative research process. JSI and UNICEF Nepal hed a 2-day workshop that provided an overview of the JTHI, behaviourally informed key informant interview tools, and field data collection methods. The workshop was followed by a 3-day training course on the HCD process, as well as on-site coaching to the DH-KUSMS team. In addition, JSI and UNICEF Nepal conducted training on social and behaviour change approaches and interpersonal communication (IPC) for the DH-KUSMS team, government agency representatives, other academics, health workers, and FCHVs. Reportedly, applying the JTHI to a real-life scenario helped increase the DH-KUSMS team engagement and interest in the process, serving both as a means for learning and as actual analysis and use of the formative data. Furthermore: "Engaging stakeholders through an academia-hosted network was an effective way to demonstrate the value of applied behavioral science in relation to immunization and generate stakeholder buy-in and commitment."
As reported here, this process "provided invaluable insights that could not have been captured without an iterative, participatory process. In addition, this approach has led to changes among BSC members in the way they are thinking about immunization service delivery. Members are looking at persistent challenges within the health system and are asking to use applied behavioral science to address them. For example, one member asked: 'How can we make health services available 24 h a day? To do this, we need to examine behaviors of the health system and the health provider to understand what the barriers are and break them down into manageable pieces to address.' This is a reflection of the benefits of using participatory processes such as HCD to address complex real-world challenges, including increased relevance to context, better translation of research to action, and potential to lead to solutions that are more readily adopted and more effective..."
The formative research allowed the BSC to conduct evidence-based advocacy, advocating for context-specific demand programmes that are tailored to the needs of underserved communities. For example, after sharing the research findings analysed using the JTHI with the Kathmandu Municipality Health Department, the department held an emergency session to identify and immunise communities located in the last mile, promptly using behavioural insights to implement new programmes. After revisiting the same community for implementation research, the team found that many community members reported that their children had received vaccines with the assistance of the government team. Moreover, the findings from the formative research were used to advocate at the policy level during the National Immunization Strategic Planning workshop, as well as to advocate for further application of and capacity strengthening in behavioural science.
In addition, engaging government stakeholders in the selection and application of the JTHI encouraged the government to apply the tool to other challenges. For example, the Ministry of Public Health (MOHP) requested that the DH-KUSMS research team support the government's response to a measles outbreak in Nepalgunj, Banke district of Lumbini province using the JTHI and rapid inquiry approaches. Through applying these methods, the DH-KUSMS team was able to quickly identify specific behavioural and social drivers of under-immunisation that contributed to the outbreak and to work with municipal and ward-level health authorities to design tailored strategies to encourage eligible children to receive the measles vaccine during the outbreak response. These strategies included: engaging religious and ward leaders and community influencers; engaging male family members in vaccination counseling; offering door-to-door vaccination; and conducting advocacy to revise outbreak response guidelines to be inclusive of children with different abilities, ensuring equitable access.
Reflecting on the experience, the team notes that, "To institutionalize this type of application and use of behavioral science models, methods, and tools,...there is value in forming networks to develop capacity in and institutionalize the use of behavioral science....In Nepal, situating a network within an academic institution has demonstrated potential as an effective model for capacity development and application of behavioral science in immunization and broader health programming....In order to scale and sustain the capacity and use of behavioral science for public health programming, it is essential to have an institution pushing a behavioral science agenda and serving as the 'go to' entity for support within the country."
As part of its capacity development strategy, the BSC is in the process of incorporating a behavioural science curriculum for its Masters of Public Health (MPH) students. There is potential to scale this curriculum across Nepal because of KUSMS' linkages to other public health institutions in the country.
The team believes the BSC model can be replicated in other countries over a period of 3-5 years if the following are in place: (i) support for orientation and advocacy for behavioural science application, (ii) an existing institution with the interest to establish and build a behavioural science centre, and (iii) technical and operational assistance to the institution. "Once capacity is developed within countries, as the work in Nepal has demonstrated, local institutions will be able to apply behavioral science tools and methods to address global immunization priorities (i.e., reaching zero-dose children, addressing norms and behaviors that prevent vaccine uptake)."
Vaccines 2023, 11, 1709. https://doi.org/10.3390/vaccines11111709.
- Log in to post comments