











































Vaccine Hesitancy and Health Care Providers: Using the Preferred Cognitive Styles and Decision-making Model and Empathy Tool to Make Progress
Poland and Associates Consulting (Poland); Mayo Clinic (Ratishvili)
"...allows for robust conversations about beliefs surrounding vaccine acceptance and hesitancy, as well as engaging in decision-making conversations in a manner and strategy that the HCP most resonates with and understands."
Healthcare providers' (HCPs') vaccine-related knowledge, attitudes, and beliefs impact how whether and how they accept and deliver vaccines, protect themselves from disease, and act as advocates for patient immunisation. However, vaccine misinformation, hesitancy, and rejection among HCPs are an ongoing issue across both developed and developing countries. This paper explores HCP vaccine hesitancy and factors influencing their vaccination decision-making. It then proposes the use of the Preferred Cognitive Style and Decision-Making (PCSDM) model and an empathy tool to increase HCP provider vaccination rates.
To provide context for the discussion, the paper examines HCP vaccination rates, looking in particular at influenza and COVID-19 vaccines. As reported here, across a multitude of surveys conducted among HCPs around the globe, the major reasons for vaccine hesitancy/uncertainty or refusal are similar for both these types of vaccines. They include concerns about safety, possible side effects, fast-track approvals by national regulatory authorities, unknown long-term risks of getting the vaccine, lack of knowledge about available vaccines, assumed low risk of getting the disease, minimisation of actual threats imposed by the virus, and low levels of trust in government and health authorities, to list a few. Overall, the literature indicates that easy-access, free vaccination, educational campaigns, peer-based interventions and social norming, decision aids, various incentives, requirements for vaccine declination forms, and vaccine mandates have been associated with increases in HCP immunisation rates in diverse healthcare settings. Combinations of these different strategies and multifaceted approaches are likely to be more successful than any individual strategy alone.
With this background laid, the paper introduces a model that seeks to understand the preferred cognitive style(s) that an individual employs in making decisions and looks at how this impacts the choices they make. This model, called the PCSDM, emphasises that humans do not make decisions in a singular way, but instead employ a variety of different styles when making decisions. Thus, it is important for the HCP, and the medical community as a whole, to be flexible in their presentation of vaccine information, along with how they engage in conversation about vaccine fears and hesitancy, in order to present information in such a way that aligns with the preferred cognitive style of the listener (e.g., a patient or an HCP - notably, HCPs are also patients, and thus information regarding how HCPs communicate with their patients also applies to HCPs in general).
Table 1 in the paper outlines several of these common cognitive styles, their verbal expressions/phenotypes, and communication strategies that might be helpful for that style. For example, those who use "bandwagoning" might reason, "If others are refusing the vaccine there must be something to it. I'm going to skip getting the vaccine". The HCP encountering such a patient would want to understand primary influencers, point out logical inconsistencies, and use social norming and self-efficacy approaches. Likewise, instead of continuing to give information and data to patients when they reject previously given data, HCPs would be best served by getting a wider picture of the patient, their fears, where they are getting information they trust, and what their preferred cognitive style is. By doing this, HCPs are better able to develop a respectful and trusting relationship with their patient, as argued here.
In a study conducted in the United States, medical residents were randomised into two groups: one received was a fact-based curriculum and the other a PCSDM-based curriculum. At the end of the study, researchers concluded that the PCSDM-based curriculum group had significant improvements in multiple domains that assessed confidence in counseling patients on immunisations.
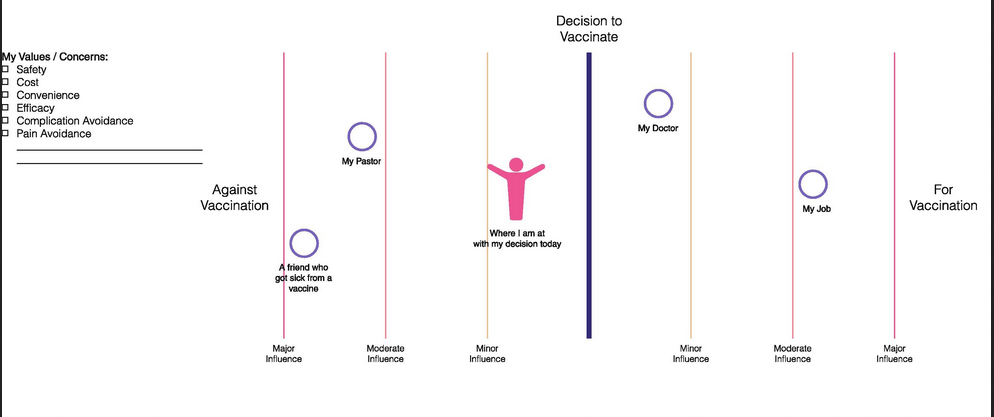
Also, in a prior publication, one of the authors outlined the use of an empathy tool (see image above) designed to help HCPs explore influences on an individual - e.g., their doctor, religious institution/pastor, friends, or favourite blogger - and how these influences impact their decision-making. This tool also helps the HCP explore an individual's values, concerns, and motivations within the decision-making process. Underlying the creation of the empathy tool is human-centred design, which aims to address a particular need through a systems-based approach. The empathy tool can also be applied to the exploration of the influences on HCP's beliefs and decision-making in regard to vaccines.
The PCSDM and empathy tool can be used in tandem, as argued here. For example, an HCP could use the empathy tool in conversation with a patient (having them identify their values, fears, motivations, and concerns, as well as to identify who their primary influencers are). Throughout this conversation, the HCP can be listening for particular statements that identify the preferred cognitive style utilised by the patient as identified in the PCSDM table. Using this understanding of their patient's preferred cognitive style(s), the HCP can have a more robust conversation about patient concerns, fears, and values regarding health and vaccine decisions. Thus, the empathy tool and PCSDM model function as a feedback loop to inform the HCP how to best address patient concerns and fears surrounding vaccination.
The paper goes on to outline recommendations to help increase vaccine acceptance across the healthcare profession from an integrative approach:
- Interweave vaccine education (i.e., including use of the PCSDM model and empathy tool) into the educational programming that students receive while in pre-college, undergraduate, graduate, and health professions schools.
- Undertake intentional, proactive work to increase health literacy by incorporating programming into middle and high school education, prior to exposure to anti-vaccination misinformation and rhetoric. For example, build skills to differentiate between trusted and untrustworthy sources of information and between misinformation and evidence-based science.
- Devote funding to further development and testing of new and existing models, as well as integration of the models currently available. This research could include evaluating the usage of both the PCSDM and empathy tool across a variety of populations and settings globally.
- Design and implement vaccine requirements for HCPs, including differential reimbursement rates for healthcare institutions based on vaccination coverage rates in staff. ("However, care must be taken to not further aggravate mistrust in already vaccine hesitant individuals or to deepen the existing problem of staff shortages across healthcare settings if providers choose to opt out, posing an even greater risk to strained health systems.")
In conclusion: "It is important while discussing HCP vaccination rates to not view them as a monolithic group or apply 'one-size-fits-all' approaches, and thus it is essential to present information and engage in conversations in ways that align with how the HCP takes in and processes information and decisions....[S]ynergistic implementation of individualized approaches including the PCSDM is crucial for decreasing vaccine hesitancy among HCPs."
Vaccine: X, Volume 11, August 2022, 100174. Image credit: Adapted from Poland et al. with permission from Vaccine
- Log in to post comments