











































Human-Centered Design for Public Health Innovation: Codesigning a Multicomponent Intervention to Support Youth Across the HIV Care Continuum in Mozambique
Columbia Mailman School of Public Health (Mukherjee, Abrams); ICAP at Columbia University Mailman School of Public Health (Zerbe, Abrams); ICAP at Columbia University (Falcao, Vitale, De Gusmao); IDEO.org (Carey, Iaccarino, Kolada, Olmedo, Shadwick, Singhal, Weinstein); Columbia University (Abrams)
"When used with youth populations, HCD [human-centred design] legitimizes the experiences and opinions of youth, fosters youth empowerment, allows youth to invest in their communities, and addresses power imbalances between youth and adult stakeholders."
Prior evidence suggests using a combination approach that consists of biomedical, structural, and behavioural interventions is best suited for addressing the needs of adolescents and young adults living with HIV (AYAHIV). Human-centred design (HCD) is a person-based approach for developing complex, multicomponent interventions that drawing on participatory methods and community engagement. This article discusses use of the HCD methodology in CombinADO, an intervention to promote HIV viral suppression and improve antiretroviral therapy (ART) adherence and retention in care among AYAHIV in Nampula, Mozambique. Based on this experience, the researchers discuss the advantages of using an HCD approach to shape interventions that are grounded in the needs and desires of AYAHIV and that have the potential to be integrated into existing health systems.
As outlined here, HCD facilitates interdisciplinary collaboration among stakeholders with diverse backgrounds, using a structured and interactive approach to engage participants in rapid iteration cycles until they deem a concept to be viable, feasible, and desirable. Through the application of design thinking, HCD seeks to understand the diverse dynamic interconnections within a complex system to understand barriers and facilitators of implementation and scale-up. As a participatory, bottom-up, and community-driven approach, HCD facilitates empowerment and collective ownership by integrating community members into the research team. The ability to empathise is crucial for HCD and allows researchers to set aside their own assumptions and gain real insight into the needs, wants, and aspirations of the communities for/with whom they are developing interventions. This process is designed to empower communities to confront the issues that impact them most, address community resistance up front, incorporate community values to generate buy-in, and build consensus early on.
Researchers from ICAP at Columbia University, in collaboration with the Mozambique Ministry of Health and IDEO.org, undertook an initiative to use HCD in formative research to design (Phase 1) and evaluate (Phase 2) a combination intervention to improve HIV-related health outcomes among AYAHIV in Nampula, Mozambique. This article solely focuses on intervention development, which was completed in Phase 1.
The article provides an overview of the HCD approach employed by IDEO.org, followed by the findings. In brief, the HCD process involved:
- Formative design research with 26 young adults aged 19-24 years, 4 adolescents aged 15-18 years, 9 key stakeholders, 6 parents of AYAHIV, 5 healthcare providers, and 1 young social media influencer - Methods included ranking and card sort activities to understand whom adolescents and young people trusted in a variety of health-related situations, identify the most common barriers and motivators for ART adherence, and confirm or refine hypotheses. Sample finding: Participants said solutions to ART adherence must include the community as well as the individual, and adolescents preferred holistic, motivation-based approaches in addition to medication reminders.
- Synthesis of findings to generate action-oriented insights - Synthesis led to several insights at the individual, interpersonal, and community levels. These insights were developed with the emotional experience across the HIV care continuum (i.e., journey mapping) and behavioural adherence archetypes (i.e., personas) in mind.
- Ideation - Eight "how might we?" statements (e.g., "How might we destigmatise and normalise the mainstream narrative around HIV to increase retention and adherence?") inspired idea generation of hundreds of potential solutions that were then sorted, ranked, narrowed down, and mapped out across the user journey and personas that were developed during synthesis.
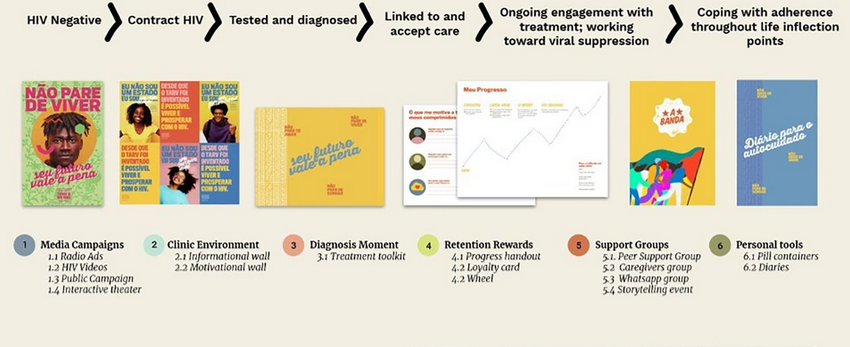
- Prototyping of intervention components - AYAHIV and healthcare providers cocreated prototypes alongside local artists and the research team. Low fidelity, rough prototypes were tested with 99 individuals. Ultimately, 12 prototypes (i.e., intervention components) spanning the HIV care continuum were selected, including: a media campaign to reduce HIV stigma and increase medical literacy; a toolkit to help providers communicate and address the unique needs of AYAHIV clients; peer-support groups to improve medical literacy, empower youth, and provide positive role models for people living with HIV; support groups for parents/caregivers; and discreet pill containers to promote adherence outside the home. Among the key learnings incorported into the prototypes were that there is a culture of secrecy and fear surrounding HIV that prevents young people and their caregivers from connecting with other people living with HIV. Thus, components were designed to promote adherence and retention in care by: fostering peer connectedness and belonging (e.g., peer support); providing accessible medical knowledge (e.g., youth-friendly clinic experience); demystifying and destigmatising HIV; and cultivating a sense of hope among AYAHIV (e.g., community empathy building).
- Pilot study - Each intervention component was piloted at 2 urban health facilities in Nampula over 12 weeks (July 2020 - October 2020). Cross-sectional data were collected to evaluate acceptability, feasibility, and uptake of each component using direct observations (n=24) and exit interviews (n=74) following: clinical consultations with AYAHIV; semistructured interviews with AYAHIV (n=42), healthcare workers - HCWs (n=4), and key informants (n=2); focus group discussions; and quantitative surveys with clients at each health facility (n=60). Based on recommendations from all pilot participants, future implementation should consider: increasing privacy in the consultation rooms so that AYAHIV are more comfortable using the CombinADO tools, communicating that wait times may increase as HCWs become familiar with CombinADO tools during consultations, facilitating communication between health facilities engaged in the study to share best practices, and addressing the needs of AYAHIV with low literacy. Prototype-specific recommendations included changes to design elements, such as changing colours, adding clarifying language or additional inspirational messaging, and including real people to increase credibility.
In Phase 2, a cluster-randomised control trial will be used to evaluate the effectiveness of the CombinADO intervention in increasing retention in care, ART adherence, and viral suppression at 12 health clinics in Nampula.
Reflecting on the process to date, organisers assert that this study "demonstrates the utility of using HCD to cocreate a multicomponent intervention to promote adherence and retention in care for AYAHIV....Although HCD methodologies can be used with nearly any population, they may be particularly well-suited for youth-driven intervention development. HCD provides a framework for cocreating interventions in collaboration with youth by incorporating lived experiences and provoking empathy and mutual understanding of the root causes of a problem within the larger socioecological environment."
As suggested here: "Public health practitioners should consider how HCD provides a pathway for public health innovation, shortens the research to practice gap, engages marginalized communities, and integrates novel interventions into existing complex systems when coupled with other synergistic research methods such as implementation science."
In conclusion, "this article demonstrates a creative process embedded in a traditional research study. HCD can serve as a community engagement model by incorporating community values, generating buy-in, and building consensus and collective ownership early on....[T]he HCD process ensures that intervention development (or adaption) is grounded in contextual needs, assumptions are tested early, and that concepts are rapidly iterated upon and refined before resources are dedicated to implementation and scale-up."
Global Health: Science and Practice 2022, vol. 10, no. 2. https://doi.org/10.9745/GHSP-D-21-00664
- Log in to post comments